
Dr Jo · FollowJust another physician
Feb 1Can asymptomatic carriers of SARS-CoV-2 (COVID-19) obtain serious lung damage? Why or why not?
Hi Bo
This is what really pisses me off about Quora. When I joined several years ago, it was because I could obtain high-quality answers to tricky questions, and contribute a bit from my own experience and insights.
Now everyone’s an expert, particularly when it comes to SARS-CoV-2. Thirty-five answers to your question, and most of them along the lines of:
“Well, D’Oh, if they’re asymptomatic it means they can’t have severe | substantial | any significant lung damage”.
Tallying these I get:
“Naah, don’t worry” [or equivalent]: 25
Vague and/or equivocal: 6
Correct: 4
Well done Joey Ortiz, Bob Whitcombe, Don Eamon, and Jim Trader. But what really disturbs me is the upvotes: just ONE upvote among all of the correct answers.
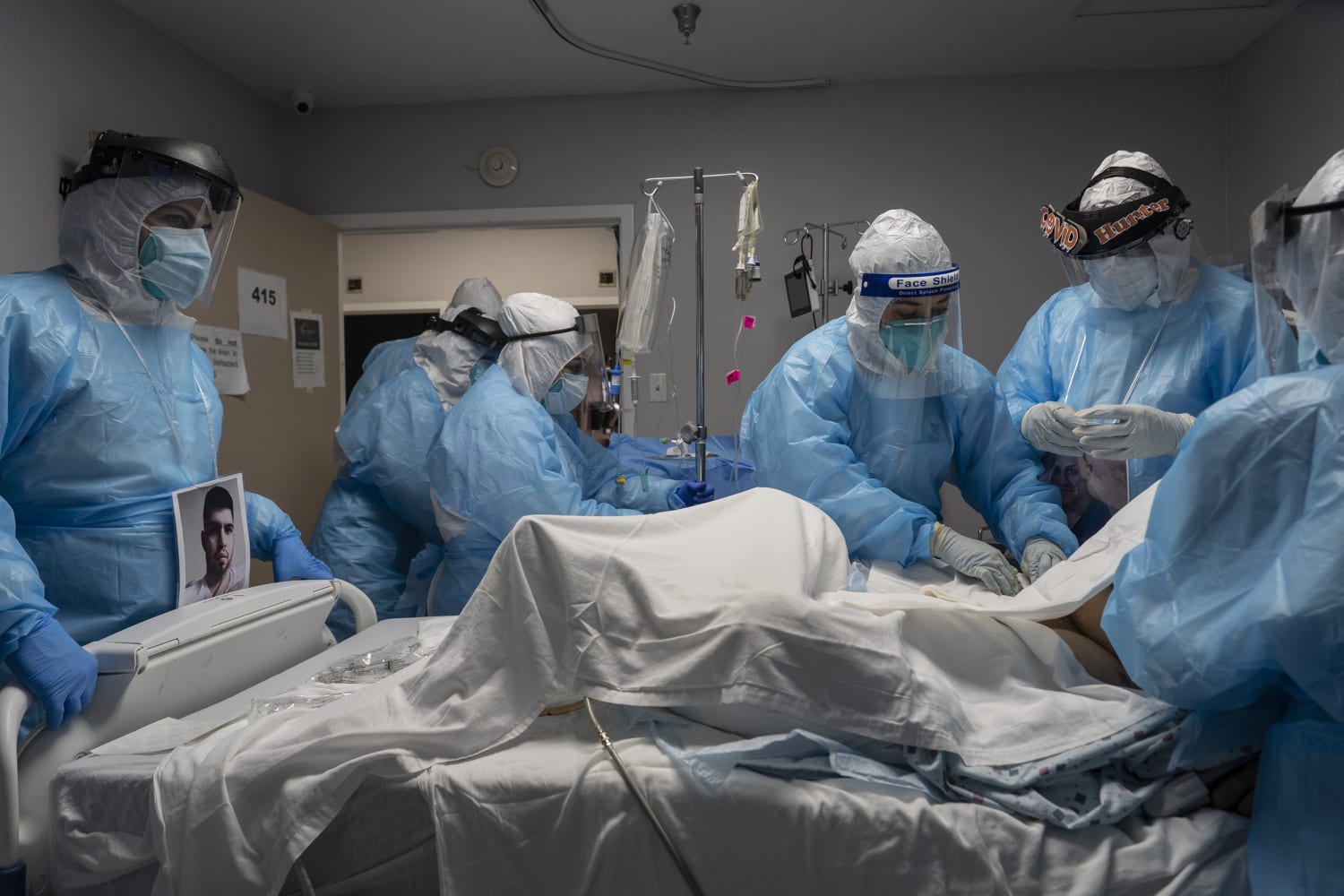
In Medicine, a symptom is something someone complains of. Something like pain or dyspnea (“shortness of breath”).* You can actually have fairly severe disease and still be asymptomatic. With COVID-19, we already knew early on[1] [2] [3] that some asymptomatic (or minimally symptomatic) patients had “walking pneumonia”.
We’ve now learned a bit more about this. It takes a fair bit of lung injury to drop the oxygen level in your blood (hypoxemia), yet some patients with hypoxemia are still asymptomatic. In a recent study from France[4] the authors found that 1107 of 1712 patients were not short of breath, but 68% of these still had pneumonia on CT scan. Not all of these had blood gas analysis, but 161 did—and 96 of these had abnormal blood gas analysis. One-third ended up in ICU, and one-quarter died.
Tobin and colleagues[5] have even said:
Patients with coronavirus disease (COVID-19) are described as exhibiting oxygen levels incompatible with life without dyspnea. The pairing—dubbed happy hypoxia but more precisely termed silent hypoxemia—is especially bewildering to physicians and is considered as defying basic biology.
Similar events got into the New York Times in April, 2020.[6] (As an aside, it’s not just the lungs either. Gupta and Mitra expressed concern[7] that asymptomatic patients are suffering cardiovascular complications too). Asymptomatic hypoxemia is however not unique to COVID-19.[8] That’s why pilots at altitude are at enormous risk—some may be happy right up until the time they go unconscious.[9]
Some patients may have no symptoms whatsoever. However, as Meyerowitz and colleagues[10] point out, some ‘asymptomatic’ cases may have been inadequately assessed. Some with positive serology may not recall their past symptoms well. Some may be ‘pre-symptomic’ and go on to develop symptoms as they become sicker—and even end up dying.[11] But people can still have severe COVID-19 without symptoms. They may also have extensive pneumonia but no more than mildly low oxygen saturation.[12]
So, before you answer a question on Quora with “It’s obvious…” why not try to find a few references that support your answer? Following this with the question “Do I actually know anything about this field?” may also be quite helpful.
My 2c, Dr Jo.
*Sometimes there can be associated signs for example tachypnoea (fast breathing), or cyanosis (going blue), an indication of lowered saturation of haemoglobin, due to decreased oxygen getting into the blood.
Footnotes
[1] Asymptomatic SARS-CoV-2 Infection and COVID-19 Mortality During an Outbreak Investigation in a Skilled Nursing Facility
[2] COVID-19 pneumonia: different respiratory treatments for different phenotypes?
[3] Case Report: Walking Pneumonia in Novel Coronavirus Disease (COVID-19): Mild Symptoms with Marked Abnormalities on Chest Imaging – PubMed
[4] Asymptomatic hypoxia in COVID-19 is associated with poor outcome
[5] Asymptomatic hypoxia in COVID-19 is associated with poor outcome
[6] Opinion | The Infection That’s Silently Killing Coronavirus Patients
[7] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7797272/
[8] “Silent” Presentation of Hypoxemia and Cardiorespiratory Compensation in COVID-19
[9] Do not go gentle: the harsh facts of hypoxia
[10] Towards an accurate and systematic characterisation of persistently asymptomatic infection with SARS-CoV-2
[11] Possible silent hypoxemia in a COVID-19 patient: A case report
[12] High COVID-19 mortality in the UK: Lessons to be learnt from Hubei Province – Are under-detected “silent hypoxia” and subsequently low admission rate to blame?


The Staggering Number of Kids Who Have Lost a Parent to COVID-19
Read in The Atlantic: https://apple.news/AQiU6udpBQhyiVP4ll7-1Hg
The Staggering Number of Kids Who Have Lost a Parent to COVID-19
Even if children are less vulnerable to the coronavirus, they don’t suffer any less from the loss it causes.By Joe Pinsker
Throughout the pandemic, media outlets and online dashboards have provided constant updates on the number of people who have died from COVID-19. Far less prominent—but just as striking—are the tallies of those left behind.
MAKE YOUR INBOX MORE INTERESTING
Each weekday evening, get an overview of the day’s biggest news, along with fascinating ideas, images, and people.
According to an estimate published recently in the journal Pediatrics, at least 140,000 American children had lost a parent or caregiver because of the coronavirus by the end of June—meaning that one of roughly every 500 children lost one of the most important adults in their life. Susan Hillis, a co-author of the study and an epidemiologist at the CDC, told me that as of earlier this month, the total had reached at least 170,000.
Fully grasping this complicates some of the standard narratives about the tragedy of the pandemic. It is not only the number of lives cut short by COVID-19 that should mark the scope of our losses, but also the millions of people who had a loved one die. And it is not just older Americans who suffer—even if kids are less vulnerable to the virus itself, they are no less vulnerable to the loss it causes.
In a typical, non-pandemic year, many children lose a parent, but globally, an additional 1.5 million children were estimated to have lost a parent or caregiver from March 2020 to April 2021. And in the U.S. alone, the number of people who have lost a close relative—whether a child, sibling, spouse, parent, or grandparent—to COVID-19 is thought to be about 6.5 million.
Read: 4 numbers that make the pandemic’s massive death toll sink in
RECOMMENDED READING
- Why Parents Kept Their Kids Home From SchoolJESSICA MCCRORY CALARCO
- Fear of COVID-19 in Kids Is Getting Ahead of the DataLUCY MCBRIDE
- SPONSOR CONTENTCreate a Personal Main Street of Small BusinessesFACEBOOK
For children in particular, the death of a caregiver is tremendously destabilizing. “It essentially shatters kids’ assumptions about the world when their parents—these figures who are supposed to provide a sense of security and safety and meet basic needs—die,” Tashel Bordere, a professor of human development and family science at the University of Missouri, told me. Many kids who lost a parent during the pandemic will continue living in the same home, but some will move in with another family member or close friend. Others will enter the foster-care system or become homeless.
The racial disparities among this group are stark. According to the Pediatrics study, Hispanic children have been almost twice as likely as white children to lose a caregiver because of the pandemic, Black children have been more than twice as likely, and American Indian and Alaska Native children have been more than four times as likely. Hillis told me that these inequities reflect the facts that Americans of different races have died of COVID-19 at different rates and have different fertility rates.
Bordere said that the way children respond to death can vary based on their developmental stage, gender, and personality, among other factors. But in general, children who lose a parent tend to be at higher risk of experiencing physical- and mental health problems, housing instability, academic and behavioral issues, and sexual abuse. They are also more likely to enter poverty—for many, a parent’s death means a loss of income.
The passing of a sole caregiver who’s a grandparent can be especially hard, because it represents a “double loss,” after the earlier death of or separation from a parent. (Approximately 10 percent of American children live with a grandparent in their household; that rate is higher for Black, Hispanic, and Asian children.)
A caregiver’s death during a pandemic presents unique challenges for grieving kids. Job instability and general stress may have depleted the abilities of other adults in their lives to support them. And they have to live with constant reminders, in the media and daily life, of why their parent is gone. “[The] replaying of an event can retraumatize children,” Bordere said. “The masks, the numbers that we’re updated on—anything related to COVID will be a trigger for a child who has dealt with a loss.”
Not every child even gets room to process their emotions. Bordere told me that Black children are frequently penalized in school for perfectly normal reactions to death, such as crying, distractedness, and fatigue. This punishment can impede their grieving process. In a study from before the pandemic, Black Americans were found to be more likely than white Americans to have experienced a death in their family during childhood.
And children in general may struggle more than adults with how inexplicably the virus arose and with not getting to be present for the end of their parent’s life. “Children are imaginative, particularly younger children,” Bordere said. “They’re left with [mental] images that may be far worse” than what actually happened in their parent’s final days.
What would help these children? “We’ve learned that programs that target one type of vulnerable child (e.g., an ‘AIDS orphan’ or ‘COVID orphan’) can be highly stigmatizing and inefficient,” Rachel Kidman, a social epidemiologist at Stony Brook University, wrote to me in an email. Instead, she suggested anti-poverty initiatives and additional resources for counseling in schools—“programming that is more universal, but still sensitive to the needs of these children.”
These children don’t match the oversimplified portrait of a typical COVID-19 victim: an old person near the end of their life. But the coronavirus can also have awful effects on people at the very start of their lives, even when they themselves don’t get sick. “For every surge in COVID cases, until we have widespread, adequate vaccination, there will be a surge in COVID deaths,” Hillis told me. “And for every surge in COVID deaths, there will be a surge in COVID orphanhood.”

ARS TECHNICA: No, your antibodies are not better than vaccination: An explainer
Read in Ars Technica: https://apple.news/

Doctors grow frustrated over COVID-19 denial, misinformation
HEATHER HOLLINGSWORTH ` October 4, 2021, 11:19 AM
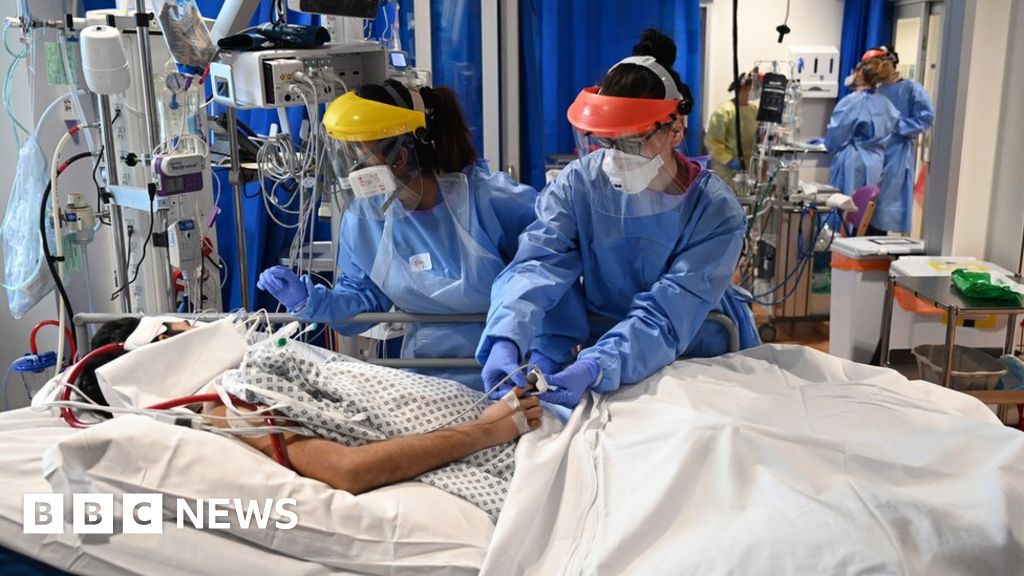
The COVID-19 patient’s health was deteriorating quickly at a Michigan hospital, but he was having none of the doctor’s diagnoses. Despite dangerously low oxygen levels, the unvaccinated man didn’t think he was that sick and got so irate over a hospital policy forbidding his wife from being at his bedside that he threatened to walk out of the building.
Dr. Matthew Trunsky didn’t hold back in his response: “You are welcome to leave, but you will be dead before you get to your car,’” he said.
Such exchanges have become all-too-common for medical workers who are growing weary of COVID-19 denial and misinformation that have made it exasperating to treat unvaccinated patients during the delta-driven surge.
The Associated Press asked six doctors from across the country to describe the types of misinformation and denial they see on a daily basis and how they respond to it.
They describe being aggravated at the constant requests to be prescribed the veterinary parasite drug Ivermectin, with patients lashing out at doctors when they are told that it’s not a safe coronavirus treatment. An Illinois family practice doctor has patients tell him that microchips are embedded in vaccines as part of a ploy to take over people’s DNA. A Louisiana doctor has resorted to showing patients a list of ingredients in Twinkies, reminding those who are skeptical about the makeup of vaccines that everyday products have lots of safe additives that no one really understands.

Here are their stories:
LOUISIANA DOCTOR: ‘Just stop looking at Facebook’
When patients tell Dr. Vincent Shaw that they don’t want the COVID-19 vaccine because they don’t know what’s going into their bodies, he pulls up the ingredient list for a Twinkie.
“Look at the back of the package,” Shaw, a family physician in Baton Rouge, Louisiana. “Tell me you can pronounce everything on the back of that package. Because I have a chemistry degree, I still don’t know what that is.”
He also commonly hears patients tell him they haven’t done enough research about the vaccines. Rest assured, he tells them, the vaccine developers have done their homework.
Then there are the fringe explanations: “They’re putting a tracker in and it makes me magnetic.”
Another explanation left him speechless: “The patient couldn’t understand why they were given this for free, because humanity in and of itself is not nice and people aren’t nice and nobody would give anything away. So there’s no such thing as the inherent good nature of man. And I had no comeback from that.”
People who get sick with mild cases insist that they have natural immunity. “No, you’re not a Superman or Superwoman,” he tells them.
:no_upscale()/cdn.vox-cdn.com/uploads/chorus_asset/file/22313554/GettyImages_1231219174.jpg)
He said one of the biggest issues is social media, as evidenced by the many patients who describe what they saw on Facebook in deciding against getting vaccinated. That mindset has spawned memes about the many Americans who got their degrees at the University of Facebook School of Medicine.
“I am like, ‘No, no, no, no, no.’ I shake my head, ‘No, no. That is not right, no, no. Stop, stop, just stop looking at Facebook.’”
DALLAS ER DOCTOR: Baffled at how he’s ‘lost all credibility with anti-vaccine patients
Dr. Stu Coffman has patients tell him they are scared about vaccine side effects. They don’t trust the regulatory approval process and raise disproven concerns that the vaccine will harm their fertility. He said the most unexpected thing someone told him was that there was “actually poison in the mRNA vaccine” — a baseless rumor that originated online.
He is confounded by the pushback.
“If you’ve got a gunshot wound or stab wound or you’re having a heart attack, you want to see me in the emergency department,” he said. “But as soon as we start talking about a vaccine, all of a sudden I’ve lost all credibility.”
He said the key to overcoming hesitancy is to figure out where it originates. He said when people come to him with concerns about fertility, he can point to specific research showing that the vaccine is safe and their issues are unfounded.
But he says there’s no hope in changing the minds of people who think the vaccines are laced with poison. “I’m probably not going to be able to show you anything that convinces you otherwise.”
And he thinks he could change people’s minds about the vaccine if they could follow him around for a shift as he walks past the beds of the sick and dying, almost all of whom are unvaccinated.

KENTUCKY: Political views come into clear focus after diagnosis
Dr. Ryan Stanton recently had a patient who began their conversation by saying, “I’m not afraid of any China virus.” From that point on, he knew what he was up against in dealing with the patient’s politics and misguided beliefs about the virus.
Stanton blamed people like far-right conspiracy theorist Alex Jones for spreading some of the misinformation that has taken root among his patients. Among them is that the vaccine contains fetal cells. Another said it “is a simple fact that the vaccine has killed millions.”
“In fact,” he said, “that couldn’t be more wrong.”
It’s tough to watch, especially after living through the early surges. On his worst shift last fall, an elderly nursing home patient arrived, close to death. She hadn’t seen her family in months, so staff wheeled her outside in the ambulance bay so her relatives could say their goodbyes from 20 feet away. He snapped a picture of the scene so he could remember the horror.
There was hope after the vaccines arrived, but then came the delta variant and a slowdown in immunizations.
“Really it amazes me the number of people who have this huge fear, a conspiracy theory about vaccines and will honest to God try anything, including veterinary medicine, to get better,” said Stanton.
MICHIGAN PULMONOLOGIST: Facebook post unleashes his frustration
For Trunsky, the vaccine pushback grew so intense that he turned to Facebook to describe the ire he confronts on a daily basis at his hospital in Troy, Michigan. The post listed eight encounters he had in the two previous days alone in which COVID-19 patients explained misinformation-fueled reasons for not getting vaccines or made demands for unproven treatments.

Example No. 5 was a patient who said he’d rather die than take the vaccine. Trunsky’s response: “You may get your wish.”
He has heard a litany of misinformation about the vaccine: They say it’s not proven and only experimental when in fact it is not. Others tell him the vaccine is a “personal choice and that the government shouldn’t tell me what to do.” He also has heard patients tell them they are too sick and didn’t want to risk the side effects of the vaccine. One young mother told him she wasn’t vaccinated because she was breastfeeding, although her pediatrician and obstetrician urged her it was safe. She had to be hospitalized but eventually got a shot.
Others, though, take out their anger on health care providers. Some threaten to call attorneys if they don’t get a prescription for Ivermectin, commonly used by veterinarians to kill worms and parasites. The drug can cause harmful side effects and there’s little evidence it helps with the coronavirus.
He estimates that he has cared for 100 patients who have died since the pandemic began, including the man who threatened to walk out of the hospital.
ILLINOIS FAMILY PHYSICIAN: Traces misinfo back to the Scripture, Nicki Minaj

Dr. Carl Lambert hears lots of wild misinformation from his patients. Some come from the Old Testament, some originate from the rapper Nicky Minaj.
Some of it is the stuff of internet conspiracy theories, like there’s a chip in the vaccine that will take over their DNA.
“Impossible scientifically,” says the family physician in Chicago. He also hears patients tell him that the vaccine will weaken their immune systems. He responds: “Immunology 101. Vaccines help your immune system.”
Recently he received a flurry of messages from patients who were worried about damage to their testicles — a rumor he ultimately traced back to an erroneous tweet Minaj alleging that the vaccine causes impotence.
“And I was like, ‘That’s outlandish. That’s a bit outrageous.’ So a lot of just kind of counseling that I did not expect to have to do.”
Some of the misinformation is delivered from the pulpit, he said. People have sent him sermons of preachers saying the vaccine is “ungodly or there’s something in it that will mark you,” a reference to a verse in Revelation about the “mark of the beast” that some Christians cite in not getting vaccinated.
“There’s a mixture of like almost fear … and saying, “Hey, if you do this, maybe you’re not as faithful as you should be as, say, a Christian.'”

Most common, though, is patients just wanting to wait, uneasy with how quickly the vaccine was developed. But he warns them, “Please do not try to wait out a pandemic. A pandemic will win.”
He said his job is “a lot of just dismantling what people have heard,” answering their questions and reassuring them that “vaccines work like this just like when we were kids.”
He has had some luck lately in changing minds. “I’ve had patients that maybe four months ago said ‘You are wasting your time. Dr. Lambert, I don’t want to hear you talking about it.’ And they’ll come back and say, ‘Hey, you know what? I’ve been watching the news. I’ve seen some stuff. I think I’m ready now.’
UTAH DOCTOR: Fear of vaccine side effects, then fear of dying
When Dr. Elizabeth Middleton talks to COVID-19 patients about why they aren’t vaccinated, they often cite fear of side effects. But as they get sicker and sicker, a different sort of fear sets in.
“They sort of have this sinking look about them, like ‘Oh, my God. This is happening to me. I should have been vaccinated,’” said the pulmonary critical care doctor at the University of Utah hospital in Salt Lake City.
She hears often that the vaccine was developed too quickly. “Who are you to judge the speed of science?” she wonders.
Also frustrating is the idea among some patients that there is a “secret agenda” behind getting vaccinated.
“‘There must be something wrong if everyone is forcing us to do this or everyone wants us to do this,’” patients tell her. “And my response to that is, ‘They are urging you to do it because we are in an emergency. This is a pandemic. It is a national and international crisis. That is why we are pushing it.’”
Getting through to patients and their families is a “delicate line,” she says. She tries not to disrupt the patient-doctor relationship by pushing vaccines too hard. But often the people who have been on ventilators need no convincing.
“They are like, ’Tell everyone that they have to be vaccinated. I want to call my family. They need to be vaccinated.’”

I AM A NURSE IN A LEVEL 1 TRAUMA CENTER HOSPITAL
There are five levels of trauma care—the highest is level 1. That designation means that the hospital is capable of providing total care for every aspect of injury. It’s where the most seriously injured are taken and patients that are critically injured are transferred. There are two level 1 TCs in Oregon, both are in Portland. We get patients from all over Oregon. There is a well-developed patient transport system—ground, helicopters, and fixed-wing (mostly jets). The Burn Center, Cardiac, and NeuroTrauma are the Critical Care Units that I am most familiar with—NT (NeuroTrauma) has been my home for over a decade. If a patient is critically injured and it’s not a burn or a serious heart issue—NT ICU gets them. Just when I think, I’ve seen it all—a patient surprises me with a unique way to seriously injure themselves. Traffic has really picked up in trauma—in addition to the usual “hold my beer” incidents, accidents, and falls; seeing a lot more violence: knifings, gunshots, and assaults. There is just so much anger and intolerance.
A number of the nurses in our COVID CCU came from NT—we have the skills, the experience, and the reputation of being able to handle stressful situations. While we are a strong, tough bunch—we are also humans. Every human has a breaking point—it just takes some longer to break than others. Over the past 18 months, we have lost 25% of our nurses. There have been new hires but not enough to get us back to optimum staffing levels. Most of the new hires are inexperienced—there is some real potential, just not there yet. I am dividing my time between NT and ECMO. They are different types of nursing —it keeps me on my toes. I am also precepting less experienced NT trauma nurses. I am routinely working 7-8 shifts in a row then 6-7 days off. It takes me longer to recover and then I need to cram a week’s worth of chores into three days. I never really feel rested or refreshed—just less tired and not as stressed.
Disinformation spreads like a virulent fungus through the ranks of the anti-vaxxers, anti-maskers—those that believe COVID is a hoax—those that will eat horse wormer, gargle Betadine, huff hydrogen peroxide. I am an advocate of the vaccine but no longer try to convince anti-vaxxers because it’s hopeless. Currently, methicillin-sensitive Staphylococcus aureus or MSSA pneumonia is a common occurrence for intubated patients in our COVID CCU and ECMO. It’s an opportunistic infection that occurs in post-infection COVID patients. It’s also called necrotizing pneumonia because the lungs actually die—it has a particular odor, the smell of death.
Some nights when I get home after a particularly brutal day, my thoughts go to a dark place. Why are we trying so hard to convince people to get vaccinated? The quicker the unvaccinated catch COVID, the sooner they are removed from the equation and the pandemic will end, finally. There are actually folks telling those infected with COVID not to go into the ICUs. It’s ill-advised but actually pragmatic in a cruel way. Our health care system is being overwhelmed with unvaccinated patients—following this advice would certainly reduce the overcrowding. Currently, about 50% of our COVID CCU and ECMO patients are dying—the DELTA variant combined with the MSSA pneumonia appears to be a significant contributor. That my thoughts would even go to such a repugnant place is disturbing. Just another reminder that I have changed.


